Is foot or ankle pain keeping you from doing what you want? Don’t let your pain keep you on the inside looking out.
At Stadia Sports Medicine, we are performing a revolutionary procedure that is changing the lives of our patients for the better.
Tenex Health TX offers a safe, quick, minimally invasive solution to relieve pain, restore mobility, and rapidly return patients to their normal activities. The procedure is performed in less than 20 minutes, patients are awake and alert throughout (only a local anesthetic is used), and no sutures or stitches are needed—only a small adhesive bandage is required. Most patients are able to return to normal activity within 6-8 weeks. Call us at 515.221.1102 or email us at reception@stadiasportsmedicine.com today for more information about Tenex Health TX. Maybe it’s time to move forward and leave the pain behind.
Dr. Carlson was one of the first doctors in our area to be trained on this groundbreaking technology.
Is your pain interfering with your work, your play or simply living your life?
- Quick pain relief
- Rapid return to normal activities
- Local anesthetic used instead of general anesthesia
- No sutures, no stitches (requires only a small, adhesive bandage)
- Minimally invasive, not open surgery
- Covered by most insurances
We are here for you…
Questions and Answers:
- Achilles tendonitis
- Patellar tendonitis (“Jumper’s knee”)
- Plantar fasciitis
- Rotator cuff tendonitis
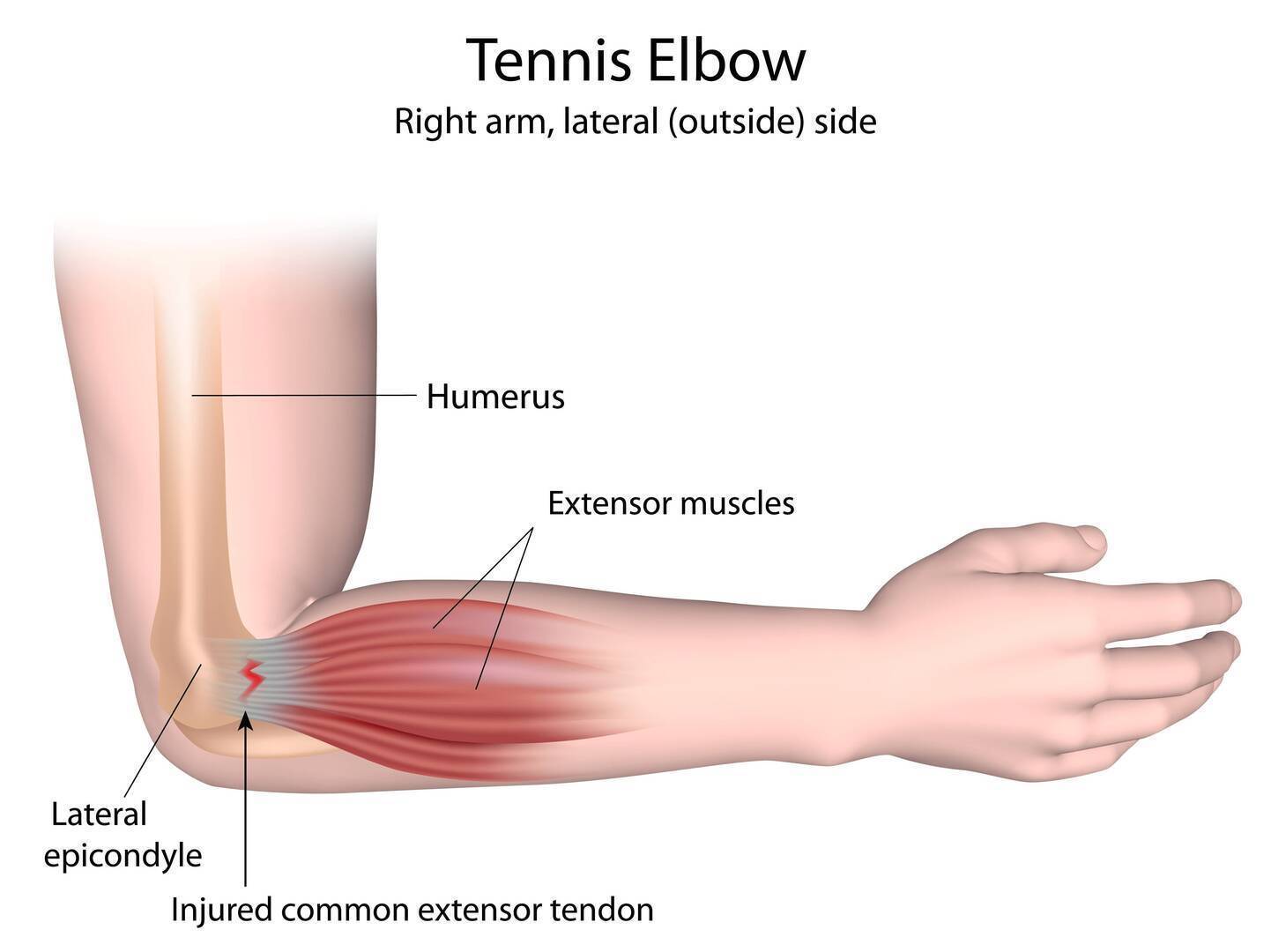
- Tennis elbow
- Golfer’s elbow
- Cutting-edge Physical Therapy
- Stadia Sports Medicine was the first clinic in Des Moines to utilize the ASTYM technique with our patients, having used it since our opening in 2006. ASTYM was developed by Dr. Carlson’s fellowship director at Ball State University in Muncie, Indiana, Tom Sevier, M.D., who went on to found Performance Dynamics
–the company that trains clinicians in the ASTYM technique. Thus, practitioners at Stadia have experience
with ASTYM going back to the 1990’s, and our therapy staff has a broader depth of experience with this technique than any other physical therapy group in Des Moines. - Stadia Sports Medicine’s physical therapists also utilize the latest in therapy techniques designed to speed tendon healing and promote more rapid recovery from injury. We do not rely on techniques such as electrical stimulation or therapeutic ultrasound which are commonly used in therapy settings but which
have not been shown to be effective for these problems. Our approaches to patients are grounded in
the medical literature.
- Stadia Sports Medicine was the first clinic in Des Moines to utilize the ASTYM technique with our patients, having used it since our opening in 2006. ASTYM was developed by Dr. Carlson’s fellowship director at Ball State University in Muncie, Indiana, Tom Sevier, M.D., who went on to found Performance Dynamics
- Injection therapies – Injection treatment can take one of several different approaches, including:
- Steroid injections – Steroid injections reduce pain and swelling associated with chronic tendon injury. Although steroid cannot be directly injected into tendons, it can be injected around the tendons themselves in order to provide pain relief. This is best done under guidance, both to ensure a good response and to minimize procedural pain. Steroid injections can assist the rehabilitation process. They are covered by almost all insurance plans.
- Prolotherapy – Prolotherapy involves the injection of an irritant substance into an injured tendon with the goal of stimulating a healing response. Although different substances can be used, at Stadia, we utilize Dextrose – a form of sugar – because of its safety profile and use in studies that have shown a clinical
benefit to patients. In the case of prolotherapy, dextrose is injected directly into the tendon in the area of
injury, with guidance utilized to promote precision of placement. Although prolotherapy is not a covered
benefit for most insurance plans, it’s low expense makes it a feasible option for most patients. - PRP (Platelet-rich plasma) injections – PRP involves the injection of a patient’s own blood into an area of tendon (or joint) injury. Specifically, the blood is prepared prior to injection by being spun in a centrifuge so that the platelets can be isolated for injection. Platelets contain many factors in them that promote wound and tissue healing. PRP shows promise as a useful therapy when more conservative measures have failed. At Stadia we utilize the Harvest PRP system, which provides an optimal concentration of platelets for injection to the injured area – something that has been shown to be important for optimal response. We also utilize guidance for all PRP injections, to increase the likelihood of a good response to treatment. PRP is not a covered benefit for most insurance plans and is usually considered a cash service, payable at the time of the procedure.
- Percutaneous tenotomy – Click to find out more about this treatment.
- Surgical tenotomy – Used to remove the scar tissue, surgery has been found to be beneficial. However, it is accompanied with potential side effects of general surgery, unintended damage to surrounding muscle and
tissue and a lengthy recovery period with restricted activity.
traditional non-operative measures. It involves the removal of scarred tissue from an injured tendon and can be thought of as a bridge between traditional surgical tenotomy and these non-operative treatments. This short video outlines the procedure:
Outcomes seem to mimic that of surgical treatment, with less post-procedure pain and more rapid recovery, as well as lower overall costs. There is a reported 80-90% success rate among patients not responding to conservative therapies.
control post-procedure pain. Restrictions following this procedure are going to be individualized, but general guidelines are as follows:
- Tennis/golfer’s elbow
- Light activity for the first week
- Begin gentle strengthening at two weeks
- Begin more aggressive strengthening and lifting around four weeks post-procedure
- Patellar tendonitis/Quadriceps tendonitis
- Crutch protection for the first week
- Normal weight-bearing between weeks 2-4
- Progress into monitored exercise starting at four weeks post-procedure
- Achilles tendonitis
- Walking boot for first two weeks
- Normal daily walking between weeks 2-4
- Progress into monitored exercise starting at four weeks post-procedure
- Plantar fasciitis
- Walking boot for first 1-2 weeks
- Normal daily walking between weeks 2-4
- Progress into monitored exercise starting at four weeks post-procedure.
- Calcific rotator cuff tendonitis
- Sling for comfort for the first week
- Modified lifting/use for weeks 2-4
- Progress into monitored exercise starting at four weeks post-procedure
With thousands of procedures performed in the United States, there have been no reports of significant complications to date.
Percutaneous tenotomy is a covered benefit on most insurance plans.
conditions:
- Author: Koh, Joyce.
- Condition: Tennis Elbow
- 20 patients with chronic tennis elbow who had failed non-surgical treatment
- Post-treatment guidelines: Two weeks of activity modifications
- Follow-up at 2, 4, 12, 24 and 52 weeks post-procedure
- 19/20 patients were pain-free
- No complications
- Normalized appearance on ultrasound
- Author: Patel
- Condition: Plantar fasciitis
- 12 patients with symptoms of heel pain for >
four months- 11/12 were pain-free by six weeks and remained
pain-free at 3 and 6 months
- 11/12 were pain-free by six weeks and remained
- Author: Elattrache
- Condition: Patellar tendonitis
- 16 patients with symptoms for at least four
months, all having failed conservative treatment - 10 collegiate-level athletes
- 15/16 were pain-free by six weeks and remained
pain-free at 3 and 6 months. - All ten athletes returned to their prior level
of competition within three months.
- 15/16 were pain-free by six weeks and remained

visits during the first 90 days.